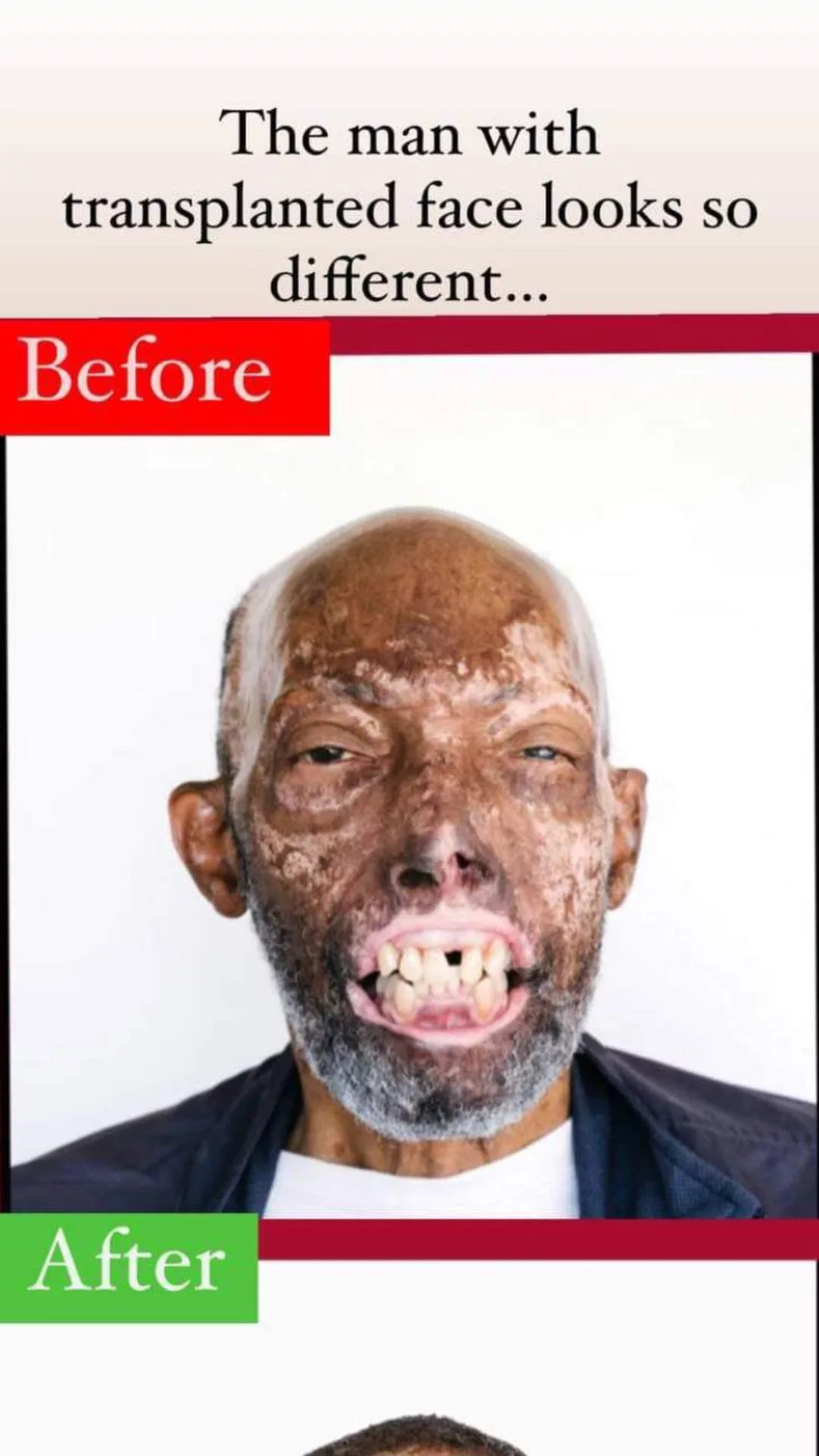
Robert Chelsea refused the first face that was shown to him as an option. It was a beautiful face, one that could have removed him off the list of candidates for a transplant after only a few short months. But Chelsea, who had suffered serious facial disfigurement as a result of a devastating car accident five years earlier, was in no rush. Because he had almost no lips, he had gotten used to leaning his head back in order to prevent liquids and food from escaping his mouth. He was able to respond empathetically to children who stood in awe and terror and stared at him. The face, which was made available in May 2018, had previously belonged to a man with skin that was far lighter than what remained of Chelsea’s. The skin was so light that Chelsea, who is of African American descent, could not handle the prospect of becoming “a totally different looking person.”
His hesitation was understood by Chelsea’s medical staff. In general, face transplants are not very common. Since the first partial one was conducted in France in 2005, less than fifty have been accomplished everywhere else in the world. It is always remarkable when a new patient joins the ranks of those being treated, but the case involving Chelsea bears considerably more weight than is typical. It is anticipated that Chelsea’s procedure would have repercussions that extend beyond his individual circumstance due to the fact that he is the first African American to have a full face transplant. The disparities in the healthcare system that cause black Americans to have greater loss rates than white Americans from a variety of conditions, including heart disease, cancer, diabetes, and HIV/AIDS, have also caused inequities in organ donation and transplantation. As a result of widespread distrust of the medical system, many African Americans are reluctant to donate tissue, which contributes to a shortage of donors. As a direct result of this shortage, just 17% of black patients who were waiting for an organ transplant received one in 2015, in comparison to approximately 30% of white patients.

It is possible that Chelsea’s unintentional role as the actual and symbolic face of black organ transplantation will contribute to the reduction of such inequities. “Having a visible, tangible reference, especially for African Americans… is so needed,” says Marion Shuck, president of the Association for Multicultural Affairs in Transplantation (AMAT). AMAT stands for the Association for Multicultural Affairs in Transplantation. According to Shuck, making one’s personal experiences public can motivate potential donors by providing a concrete illustration of the good effects that a transplant can have. Despite the rarity of facial donation, Chelsea’s tale has the potential to inspire black Americans and their families to donate organs such as kidneys, livers, or lungs, which will help save lives and cut down on wait times across the country.
It took more than a year for Chelsea to receive a second call—the one that would land him in a bed at Boston’s Brigham and Women’s Hospital, receiving a new face that was a near perfect skin-color match, and that made him both the first African American to undergo a face transplant and, at 68 years old, the oldest recipient ever. Chelsea’s new face was a near perfect skin-color match. “Morning by morning, new versions of me unfold,” Chelsea stated on the day he was freed from the hospital in August, about a month after surgery. This was nearly a month after he had undergone surgery. “[But] I feel like myself.”
On a Monday night in August of 2013, Chelsea was having difficulty with his automobile, so he pulled over to the shoulder of the highway outside of his home, which is located near Long Beach, California. Almost immediately after that, an intoxicated motorist crashed into his vehicle, causing it to burst into flames. Burns of the third degree covered over half of Chelsea, a sales manager for a company that specializes in rubber stamps, when he was taken to the hospital in an ambulance.

In the four months that followed his transfer to the University of California Irvine Medical Center, Chelsea struggled in and out of consciousness as medical professionals worked to preserve his life. In that time period, he underwent a total of 18 surgical procedures, the most of which were skin grafts to cure his burns. However, he also underwent abdominal operations to manage acute gastrointestinal issues that had developed while his body fought for its life. Because of the drugs he was taking for high blood pressure, blood flow was redirected to his heart and away from his extremities, which caused the loss of tissue in his lips, nose, and fingers. Dr. Victor Joe, who was one of his surgeons, referred to him as “one of the sickest patients we’ve had.”
Although Chelsea was able to walk away from UC Irvine in December 2013 with his life, by the time he had completed his rehabilitation, he had lost his lips, the top of his nose, many of his fingertips, and two-thirds of his intestines. His face was disfigured in deep scars, and his hands were covered in cadaver skin that matched Chelsea’s skin tone but never completely imitated its texture; Chelsea referred to the cadaver skin covering his hands as his “snakeskin.” Over the course of his life, he would finally wear the skin of three distinct individuals. Before the catastrophe, he had already helped others by donating organs; nevertheless, he had no idea how challenging it would be to replace his skin.
The walls were built long before Chelsea was even conceived of. In 1932, researchers from the United States Public Health Service began a study at the Tuskegee Institute in Alabama that would have a profound impact on the practice of medicine in the United States for many years to come. Covertly planned to allow researchers to monitor the consequences of untreated syphilis over the period of four decades, the trial was carried out in secret. Six hundred black men, most of whom were sharecroppers, signed up to participate in the research after hearing that they would receive free transportation, meals, and medical treatment if they did so. About two-thirds of the males had syphilis, and half of them were treated with arsenic and mercury, which was the conventional treatment at the time. Even after it was established in the 1940s that penicillin was an effective cure for syphilis, the other males who were infected with the disease were not given any kind of treatment. They were abandoned to either perish, pass the illness on to their partners and children, or acquire complications such as heart failure, mental instability, or blindness.
In 1972, when the Associated Press broke the story of the study, there was an immediate backlash from the public. A settlement reached in 1974 awarded around $10 million in compensation to surviving patients and the relatives of patients who had passed away. Twenty years later, in 1997, then-President Bill Clinton issued an apology for the Tuskegee experiment, describing it as “deeply, profoundly, morally wrong.” However, the cut was severe, and it would leave a scar. “African Americans still do not think that the health care profession will take care of them,” adds Shuck. ”
This suspicion was not founded just on the Tuskegee experiment. In the 1800s, it was normal practice to use enslaved people as reluctant and unanesthetized test subjects for medical research, and their passed bodies were regularly dissected. This practice continued well into the 20th century. Even after the institution of slavery was ended, black patients were frequently denied treatment at hospitals and clinics run by white people. Even when they were able to seek therapy, it was not always done in an ethical manner. Henrietta Lacks’ cervical tissue, which was malignant and rapidly replicating at the time, was taken from her without her knowledge in 1951. These cells went on to become a profitable cornerstone of medical research, kicking off a controversy that has continued for decades over informed consent and who benefits from scientific innovation. In a world where many clinicians, according to one research review from 2017, tacitly favor white patients, events like these and the countless more like them continue to be a major problem, especially in the medical field. According to Dr. Vanessa Grubbs, a nephrologist at the University of California, San Francisco, “the entire medical system follows along with the racism that the country was built upon.”
According to Dr. Damon Tweedy, an associate professor of psychiatry at the Duke University School of Medicine and the author of Black Man in a White Coat, the combination of well-known historical examples with more recent and personal accounts of mistreatment by families has left many African Americans wary of medical professionals. “There’s some remnant of that that you internalize,” he says. “There’s no getting around that.” Tweedy says that despite the fact that he is black himself, patients at his hospital have wondered if the hospital is “experimenting” on them or using them as “guinea pigs.”
Therefore, it shouldn’t come as much of a surprise that many African Americans are reluctant to volunteer for medical research, as doing so is frequently an essential initial step in the process of creating successful medicines. According to the findings of a study conducted by ProPublica on data provided by the Food and Drug Administration (FDA), in a number of clinical studies conducted for pharmaceuticals that were granted approval between the years of 2015 and 2018, less than 10% of participants were people of African descent. (The scientific community is seeking to close such gaps through projects such as the National Institutes of Health’s All of Us experiment, which is a study trying to enroll one million people from under-researched areas.) As a consequence, medical professionals today know a great deal more about white bodies than they do about black bodies, despite the fact that black Americans report higher rates of conditions such as type 2 diabetes, heart disease, and many cancers. This is largely due to centuries of structural inequities that have, among other consequences, left more than 10% of black Americans without health insurance, compared with about 6% of whites, and left 21% of black households without secure access to quality food, compared with less than thrice
It is essential to gain a grasp of this convoluted history in order to comprehend the current situation around organ donation and transplantation in the United States. It takes black patients, on average, longer to receive major organs like kidneys, lungs, and hearts than it does for white patients, which means that more black patients may pass away before they receive the necessary operations. According to data provided by the federal government, African Americans, who make up approximately 13% of the population in the United States, account for approximately 30% of the transplant waiting list. This is one reason why. On the other hand, over 65% of deceased donors are white, while only approximately 40% of people on the transplant waiting list are white Americans.
Because of the higher prevalence of chronic diseases among African Americans, there is not only a disproportionately high number of people in need of transplants, but there are also fewer living family members who are in good enough health to donate organs such as kidneys and livers. Even if they do, according to Shuck, “we don’t want to ask our family because we don’t want to put them at risk, so we languish for longer.”
According to Dr. Charles Bratton, a transplant surgeon at Loma Linda University Health who has conducted research on donor discrepancies, religious and philosophical beliefs may potentially play a part in the phenomenon. It is possible for Jehovah’s Witnesses to be dissuaded from participating in organ transplants due to their refusal to take blood transfusions. In the United States, Jehovah’s Witnesses make up 27% of the black population. Despite the fact that organ donation is permitted by the majority of religions, adherents of particular faiths, such as the Southern Baptists, may have the desire to have their corpses preserved in their whole after loss. Last but not least, persons in the United States, in contrast to those in certain European nations, are required to actively opt in to organ donation rather than opting out, which significantly reduces the number of people who donate their organs. Only 39% of black Americans and roughly 65% of white Americans have a notation on their driver’s licenses indicating that they are organ donors, respectively, according to the most current poll conducted by the federal government on opinions regarding organ donation.
“Can you see the expression that they are giving me? It’s cute. “They’re curious,” Chelsea stated when we first met in November 2018, some months before to his surgery. “They’re curious about everything,” Because it was a Monday and he typically worked out on Mondays, he instructed me to head directly from the airport to his gym in Victorville, California as soon as I landed. After that, we performed an errand at Metro-PCS and then stopped to pick up some tacos for lunch on the way home. Even though others were staring, Chelsea kept a cheerful attitude about the situation. “I don’t blame them,” was the statement that he made. “It’s terrifying. It’s almost as if I’m donning a mask for Halloween.”
Chelsea asserted, five years after his injury, that his appearance did not worry him. He attributed this assertion to the profound Christian faith that he had developed throughout the course of his recuperation, which played a significant role. In addition, he quipped that he was “no knockout looker” before the accident, despite the fact that his friends and family remember him quite differently. In point of fact, his acceptance was so unwavering that Chelsea wasn’t even sure he wanted a face transplant when it was first approved for him by Dr. Bohdan Pomahac, director of plastic surgery transplantation at Brigham Health.
The way Chelsea carried herself was remarkable. Losing one’s face, which is a person’s introduction to the world, is traumatic for the majority of people who go through it because of the psychological damage it causes. Patients who receive face transplants are expected to go through a significant amount of counseling before they can be considered ready to accept their new appearance. When one’s racial identity is also on the line, it can make things an awful lot more difficult. Although a black patient who is waiting for a kidney or heart transplant does not require a donor of the same race, a complexion match is regarded essential for visual transplants in order to preserve as much of one’s identity as is practicable.
According to Jessica DeCuir-Gunby, a professor at North Carolina State University who researches the topic but has not collaborated with Chelsea, physical appearance is not the main factor in determining racial identity, but it is undoubtedly a role. She argues that accepting a face from a donor with significantly lighter skin could bring up a complex range of feelings due to the fact that black identity can be expressed through a variety of skin tones, hair textures, and facial traits. According to her, a significant alteration in one’s outward appearance has the ability to detach a person from his or her identity, which can lead to psychological distress. A transplant psychiatrist at the Mayo Clinic named Dr. Sheila Jowsey-Gregoire, who has not worked with Chelsea, says that even though most face-transplant patients have done the difficult work of accepting that they’ll never look exactly like they did in the past, changing their racial identity could lead to unanticipated negative consequences.
The need for a precise color match further narrows an already tiny pool of possible donors: in the federal poll on organ donation, only approximately 41% of black respondents indicated they’d be at least “somewhat” eager to donate a face, but around 61% of Caucasian respondents said they’d be prepared to donate a face. Even Chelsea, who doesn’t care much about how he looks on the outside, had a hard time wrapping his head around the idea of accepting a face that was so much paler than the one he was used to seeing.
It wasn’t simply the prospect of stumbling into an unknown face in the reflection that caused Chelsea to halt. Patients who have undergone organ transplantation are need to take immunosuppressant medication for the remainder of their lives in order to prevent their bodies from rejecting the organs that were donated to them. His health had been steady in the years following his recovery from the accident, but the transplant would force him to enter a world of frequent doctor’s appointments and prescriptions once again. Even though the Department of Defense awarded Brigham and Women’s Hospital a grant to test a less cumbersome post-transplant immune-suppression regimen, Chelsea’s surgery would still be performed at no cost to his family. However, his family would be responsible for paying some of the associated costs, such as travel and caretaker costs. In the same year that NYU Langone performed the first face transplant that was covered by commercial insurance, the hospital estimated that the patient would have been responsible for paying around $1.5 million out of pocket for the procedure. Even though Chelsea’s family had no intention of shouldering any of those expenditures, they were forced to start a GoFundMe campaign in order to raise more than $75,000 in order to pay for various out-of-pocket expenses. Even more traditional transplants can be pricey. According to Tweedy, the financial hardship of becoming a living donor and recovering from an invasive operation, which often involves time off from work, inhibits lower-income patients, who tend to be disproportionately people of color, from engaging in transplants. This is because recovering from the procedure often requires time off from work.
Ebony, who is thirty years old and is Chelsea’s daughter, was much more anxious than her father. She compares the experience of witnessing him in critical condition following his accident to “going to a movie theater and watching the scariest movie that they had out, and you replayed it over and over again.” “You went through all of that, and now all of a sudden you want to come over here and [have another procedure]? There is always the risk of problems with surgery.
In the end, though, Chelsea wanted to be able to eat and drink regularly, to spit, to swallow a medication, to close his mouth, and most importantly, according to what he claimed, to kiss Ebony on the cheek. In the end, he came to the conclusion that the benefits of doing so outweighed the potential drawbacks.
According to him, it took some time before he was able to fully appreciate the significance of becoming the first African-American to receive a face transplant. When the understanding finally hit, there was a sense of unease associated with it. About six months before his operation, Chelsea expressed that while he did feel some pride, he was unsure whether or not it was something to be proud of. “There is a degree of pride, admittedly, and yet I’m not sure that it’s something to be proud of,” Chelsea remarked. “There is nothing holy about those actions,” said the speaker, “to celebrate an individual because they haven’t done anything any more than anybody else, they just happened to be there at the right time.” However, Chelsea was able to understand that the operation had a greater purpose, which was to serve as a shining example of the ways in which organ donation may transform lives, particularly those of black Americans. “We are a lot more hesitant to be a donor,” he adds. “We have a lot more doubts.” Because of this, we are at a disadvantage in the event that we require a kidney, liver, or lung.
Even after getting so close with the first face in the spring of 2013, when the hunt for a donor had been going on for more than a year, Chelsea’s surgeon remained unfazed. “All it takes is one. Pomahac made this prediction around six months before ultimately identifying the donor face that would become Chelsea’s. “Sooner or later you will find one,” Pomahac stated. Less than seven percent of the organs that were harvested in the predominately white region of New England, which is home to Brigham and Women’s Hospital, came from African-American donors in 2017. Although it is possible that Pomahac and his team might potentially accept a donor organ from any place, the policy of the hospital stipulates that the journey time to the donor site must exceed four hours. This is done in part to ensure that the organ continues to operate properly. If Pomahac and his colleagues wanted to seek outside of New England, as they eventually did, they would have to select a location that was within a convenient flight distance of Boston.
Chelsea never questioned his choice to decline the first face that he saw, but he also had no way of knowing how long the search would take. He and Pomahac had used a scale ranging from 1 to 18 to discuss the complexions of potential donors, with 1 being the lightest. According to Pomahac, Chelsea’s complexion is a 15 or 16. Initially, they looked for donors falling between the ages of 8 and 16, but after several months of fruitless searching, Chelsea eventually gave in and consented to consider donors as young as 5. Even that was not successful.
After that, in the spring of this year, Pomahac suggested to Chelsea that perhaps they might explore a full facial transplant rather than the partial one they had intended to perform, which would just replace the lower area of his face. Pomahac was primarily concerned with cosmetics, but Chelsea and his family believed that the decision would help speed up the search process by minimizing the requirement to blend exactly with Chelsea’s remaining skin. This would make flawed matches less noticeable to medical professionals. Pomahac was primarily concerned with cosmetics. Chelsea gave her assent to the whole transplant, and in July, much over a year after he had been placed on the transplant waiting list, he received the call that he had been waiting for. His medical team had discovered a patient with a skin tone that was nearly identical to his own. Only descriptions of the donor’s color, age, and medical risk factors were provided to him, and he had only one day to make the most important choice of his life before he had to fly from Los Angeles to Boston for the operation. “I had no choice but to believe,” he said on that particular day. “All I could do was keep my fingers crossed that it was a real call.”
Another man, who was located in a different state, had just finished receiving a phone call that was extremely different. James, age 51, was contacted by the Gift of Life Donor Program shortly after discovering that his brother Adrian, age 62, had passed away unexpectedly. The program inquired about the possibility of donating Adrian’s internal organs as well as his face. James was not aware of his brother’s preferences on organ donation, but after serving in the Air Force, where he claims the practice was cherished, James became a staunch advocate for organ donation. He was aware that Adrian, a skilled athlete and guitarist who enjoyed listening to Hendrix, worked in the construction industry, and was constantly “ready to light up a room,” would be interested in assisting another individual. “He would give the shirt off his back for anybody,” James says about him. James made phone calls to his other five brothers before making the decision to proceed with the donation. He found solace in the knowledge that a portion of his older brother would be “still here and on this earth, [so] he lives on.” He was completely unaware of the fact that his brother’s face would make history as the first African-American face to ever undergo face transplantation.

The face that he would receive from Chelsea was concealed from public view. But the tragedy that another family had to go through in order to pave the way for him to have a fresh start was the one topic that managed to bring him to a state of melancholy in the frantic hours before the operation.
Leave a Reply